CentoXome®
Whole Exome Sequencing
For certain patients the combination of symptoms does not allow the clinician to pinpoint a potential diagnosis. In such challenging cases, often a stepwise diagnostic strategy is chosen, which makes the testing complex, time consuming, costly and often not even conclusive. Furthermore, a delayed diagnosis may have a significant impact on the patient’s treatment and quality of life.
For these cases, the use of broad, whole exome sequencing (WES) has advantages over initially more targeted genetic testing. Whereas such targeted genetic testing focuses on a single gene or on a limited set of predetermined genes, WES testing examines all the protein coding regions in the genome (exons) simultaneously. It is estimated that most of the disease-causing mutations (about 85%) are located within the exons. This lack of bias allows to also identify disease causing mutations in unexpected genes that would be missed by targeted approaches.
CentoXome®, CENTOGENE’s whole exome sequencing service, offers an accurate and cost-effective one-step solution, with high diagnostic yield.
Click Here to know more about CentoXome®
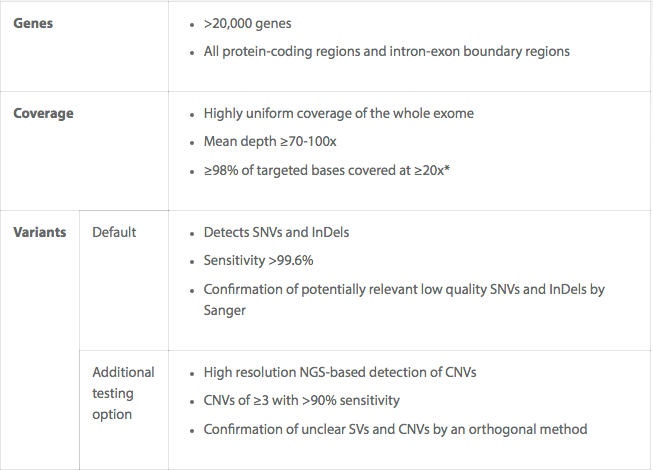
CentoXome® – Key Features
When is Whole Exome Sequencing Required?
For many patients the combination of symptoms does not allow suspecting specific genetic causes with a sufficiently high certainty. It is unclear which genes to look at.
Therefore, WES may be an affordable first test when the clinical spectrum is diverse and diagnostic answers are likely to be obtained only through sequencing the complete coding region, i.e. the whole exome. WES is also a good follow-on approach after more targeted approaches have been tried already and no causative variant was identified.
We particularly recommend WES for patients:
- With clinical or genetic heterogeneity
Examples: Epilepsy, epileptic encephalopathies, muscular dystrophies/muscular disorders, ataxia, neuropathies, cardiomyopathies, skeletal dysplasias, immunodeficiency, deafness, blindness.
- With atypical clinical presentations or phenotypes
Example: A patient presenting with intracranial aneurysm (due to PKD1 gene – polycystic kidney disease)
- With “blended” clinical presentations and clinical suspicion of dual diagnosis
Examples: Intellectual disability and severe immunodeficiency
- With clearly genetic disease, but previous genetic testing having been negative.
Example: A patient with autosomal dominant spastic paraplegia and with a negative result for the gene panel
- Who need a cost-conscious alternative to whole genome sequencing
